




There are a number of non-medication, non-therapy options for treatment-resistant depression. Somatic treatments involve stimulating electrical activity in the brain through the application of energy. Electroconvulsive therapy and transcranial magnetic stimulation are the most well-known, but there are some more obscure options as well. So let’s dive in!
Electroconvulsive therapy (ECT)
Electroconvulsive therapy (ECT) has a bad public reputation. People think it’s barbaric and much like what happened to Jack Nicholson’s character in One Flew Over the Cuckoo’s Nest. Modern ECT isn’t like that at all, though. You’re knocked out with anaesthetic, an electrical stimulus is applied to induce a seizure (electrically; there’s no physical seizure because of a muscle relaxant), and then you wake up a little while later.


ECT is the most effective treatment for depression, and it works far faster than medication, making it a good choice for people who are actively suicidal. A 2016 study found that ECT promoted neuroplasticity and growth in areas of the brain like the hippocampus and amygdala where depression had already reduced the volume compared to normal. Smaller volumes of the hippocampus prior to ECT were associated with a greater clinical response.
The biggest downside is the potential for memory loss, which is dependent in part on how many treatments you need and whether you need unilateral or bilateral placement of electrodes during the procedure. For some people it’s not an issue, for others it’s a huge problem, and there’s a whole range of territory in between. I experienced a fair bit of memory loss, but it was a price I was willing to pay for how well it works.
You can read more about ECT in the post This One Flew Over the Cuckoo’s Nest: ECT in Real Life.
Magnetic Seizure Therapy (MST)
Magnetic seizure therapy (MST) induces a seizure with a magnetic field rather than electrical current, and it’s applied to a more focused area compared to ECT. Like ECT, it is performed under general anaesthesia with a muscle relaxant. It’s a relatively new treatment that hasn’t been as well studied as ECT or TMS. It’s still unclear how effective it is compared to ECT, but it appears to cause fewer cognitive side effects.
Transcranial magnetic stimulation (TMS)

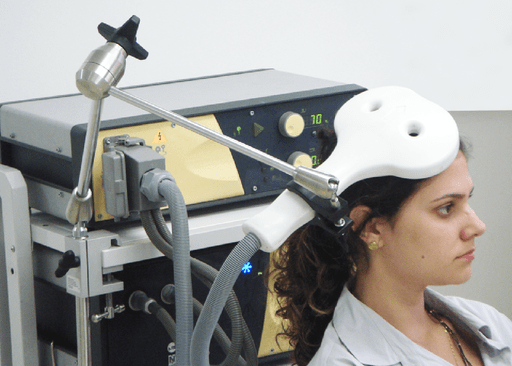
Transcranial magnetic stimulation (TMS) involves the application of a magnetic field across the brain to stimulate certain areas beneath the surface. It can help with both unipolar and bipolar depression, although it’s not as well studied in bipolar disorder. It hasn’t been found to trigger a switch to mania in people with bipolar. It doesn’t appear to be helpful in depression with psychotic features, although that hasn’t been clearly established. The more treatment refractory a patient is (e.g. if they haven’t responded to ECT), the less likely it is that they will respond to TMS, and TMS generally appears to be less effective than ECT.
There’s strong evidence to support the use of high-frequency repetitive TMS (rTMS) to the left dorsolateral prefrontal cortex area of the brain. There’s also evidence supporting the use of low-frequency rTMS in the same area on the right side, although it hasn’t been as well studied. A common method for locating the target area is to find what’s known as the hand motor hotspot, an area of the brain’s motor cortex. Stimulating this area with TMS produces a response in the muscles of the hand.
Deep TMS, which uses a different magnetic coil, is able to reach deeper brain structures than standard rTMS, which affects brain cells to a depth of 2cm below the scalp.
TMS is typically administered five days a week over 6 weeks, with sessions lasting 30-60 minutes. The patient is awake and sitting up during the treatment. Headaches are the most common side effect.
Theta burst stimulation (TBS)
Another TMS option is theta burst stimulation, which can be given as intermittent (iTBS) and continuous (cTBS) bursts. It’s administered for three minutes per session. Sometimes, an accelerated protocol is used, with multiple sessions being administered per day.
Deep brain stimulation (DBS)


Deep brain stimulation (DBS) is most often done in Parkinson’s disease, but it’s sometimes used to treat depression as well. Electrodes are implanted into the brain and connected to a neurostimulator that’s implanted below the collarbone, which generates electrical signals. Electrodes have been tried in several different areas of the brain, including the subgenual cingulate, the ventral anterior internal capsule, and the nucleus accumbens.
Getting the electrodes implanted involves neurosurgery, which can come with complications. The scary-looking image above shows implantation surgery, which involves the use of a stereotactic frame to help the neurosurgeon navigate in the brain. Magnetic resonance imaging (MRI) is used to guide and confirm placement of the electrodes. After surgery, stimulation parameters can be adjusted remotely
Because of the risk and costs associated with DBS, it tends to be used only in highly treatment-refractory cases.
Vagus nerve stimulation (VNS)


The vagus nerve, also known as the tenth cranial nerve, runs from the brain down through the neck to the heart and several other organs. Vagus nerve stimulation (VNS) involves surgery to connect lead wires to the vagus nerve, and then attach those to an impulse generator implanted below the collarbone. Settings for the impulse generator can be adjusted remotely.
It takes several months to see a therapeutic effect, and side effects are common, so it’s not used very often. Side effects include voice changes, coughing, sore throat, and hoarseness. It’s far more commonly used for the treatment of epilepsy than for treating depression.
Transcranial direct current stimulation (tDCS)


Transcranial direct current stimulation (tDCS) delivers low direct current through electrodes placed on the head, which induces electrical activity in the brain areas underneath. MRI or PET imaging may be done beforehand to determine the correct area for electrode placement. Different electrode placements have been tried in different studies, but typically, the anodal electrode is placed over or near the dorsolateral prefrontal cortex, which is the same region of the brain targeted in TMS.
The exact mechanisms by which tDCS works are still unclear, but it does appear to affect NDMA receptors for the neurotransmitter glutamate in the brain. It hasn’t been particularly well-studied in depression, but there is research evidence supporting its effectiveness.
Treatments are done five days a week for 20-30 minutes over a period of several weeks. It’s generally well-tolerated, but potential side effects include skin irritation, tingling, itching, or redness.
Cranial electrotherapy stimulation (CES)
So far, this post has covered evidence-based treatments for depression. Cranial electrotherapy stimulation (CES) deviates from that. There’s some similarity between it and tDCS, but CES uses alternating rather than direct current. This is a buy-it-online, do-it-yourself-at-home kind of deal. There’s a stimulator device and clips that you connect to your earlobes; these can run you upwards of $500.
What makes these devices a bad deal is that there’s no evidence that they work. They may be advertised as FDA approved, but when it comes to medical devices, FDA approval basically only says that they’re pretty convinced it won’t electrocute you. When it comes to CES devices, the FDA has said outright that there’s no evidence they work for depression.
Ah, good ol’ treatment-resistant depression. Never a dull moment. At least the transorbital lobotomy has gone by the wayside.

Speaking of which, this is a weird Canadian musical short film called Lotobotomobile, about lobotomist-in-chief Dr. Walter Freeman and his travelling roadshow (the roadshow existed, but it apparently wasn’t called the Lobotomobile).
Have you ever tried, or contemplated trying, any of these somatic treatments for depression?
References
- Daskalakis, Z. J., Dimitrova, J., McClintock, S. M., Sun, Y., Voineskos, D., Rajji, T. K., … & Blumberger, D. M. (2020). Magnetic seizure therapy (MST) for major depressive disorder. Neuropsychopharmacology, 45(2), 276-282.
- Eitan, R., & Lerer, B. (2022). Nonpharmacological, somatic treatments of depression: Electroconvulsive therapy and novel brain stimulation modalities. Dialogues in Clinical Neuroscience.
- Fregni, F., El-Hagrassy, M. M., Pacheco-Barrios, K., Carvalho, S., Leite, J., Simis, M., … & Brunoni, A. R. (2021). Evidence-based guidelines and secondary meta-analysis for the use of transcranial direct current stimulation in neurological and psychiatric disorders. International Journal of Neuropsychopharmacology, 24(4), 256-313.
- Joshi, S. H., Espinoza, R. T., Pirnia, T., Shi, J., Wang, Y., Ayers, B., … & Narr, K. L. (2016). Structural plasticity of the hippocampus and amygdala induced by electroconvulsive therapy in major depression. Biological Psychiatry, 79(4), 282-292.
- Lefaucheur, J. P., Aleman, A., Baeken, C., Benninger, D. H., Brunelin, J., Di Lazzaro, V., … & Ziemann, U. (2020). Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): An update (2014–2018). Clinical Neurophysiology, 131(2), 474-528.
- Rosa, M. A., & Lisanby, S. H. (2012). Somatic treatments for mood disorders. Neuropsychopharmacology, 37(1), 102-116.


Managing the Depression Puzzle takes a holistic look at the different potential pieces that might fit into your unique depression puzzle.